German Congress of Orthopaedics and Traumatology (DKOU 2025)
Loss of knee extension following ACLR and its relation to quadriceps tendon autograft diameter and notch volume
Text
Objectives and questions: Primary anterior cruciate ligament reconstruction (ACLR) using quadriceps tendon (QT) autograft may increase the risk for postoperative loss of extension (LOE), although it is unclear if this is due to a larger QT autograft diameter. The purpose of this study was to determine the association between loss of extension following primary QT autograft ACLR and QT autograft diameter while controlling for notch volume.
Material and methods: A retrospective review of a consecutive series of patients undergoing primary ACLR with QT autograft between January 2014 and December 2021 by seven fellowship-trained orthopaedic surgeons was performed. Exclusion criteria included revision ACLR, multi-ligamentous knee surgery, age <14 years, unavailable preoperative magnetic resonance imaging (MRI), and <6 months follow-up. Loss of extension was defined using the International Knee Documentation Committee (IKDC) criteria for abnormal knee extension (>5° LOE compared to contralateral) 3–12 months after ACLR, or any subsequent surgery for LOE. Notch volume was measured using preoperative MRI scans and a ratio of QT autograft diameter to notch volume was calculated. Univariate and multivariate analyses assessed factors associated with postoperative LOE.
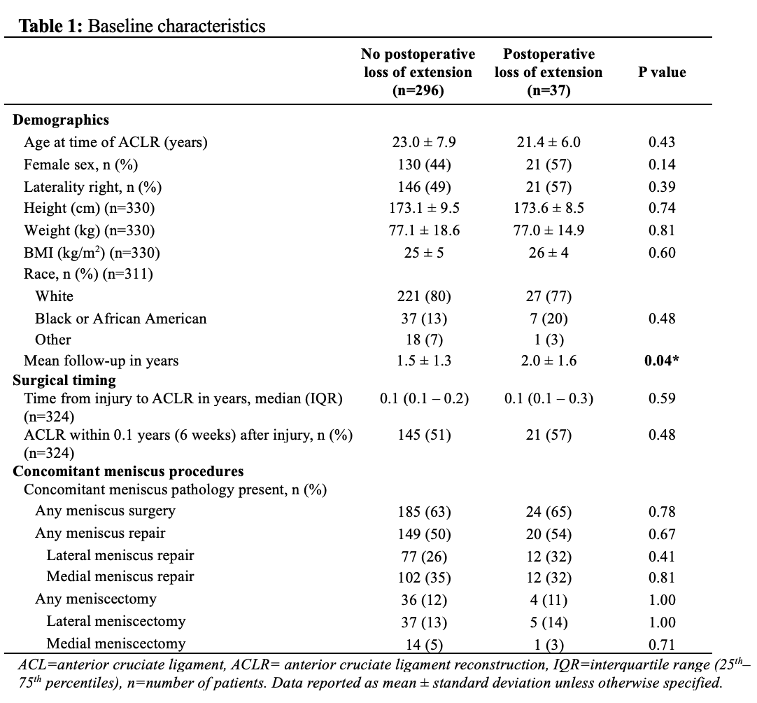
Results: A total of 500 patients were identified, of which 333 (67%) were included (mean age 22.8 ± 7.7 years, 151 (45%) female). The mean follow-up was 1.6 ± 1.3 years. The rate of postoperative LOE was 11% (n=37), and 70% (n=26/37) of those with LOE underwent a subsequent surgery to restore extension. There was no difference in QT autograft diameter (9.5 mm vs 9.6 mm, P=0.81), notch volume (6.3 cm3 vs 6.5 cm3, P=0.70), and the ratio between QT autograft diameter and notch volume (1.6 vs 1.6, P=0.75) between patients with and without postoperative LOE. Only the inability to achieve terminal extension (0°) at the initial preoperative visit was associated with postoperative LOE on multivariate analysis (OR 2.23 (95% confidence interval 1.10-4.58), P=0.03).
Discussion and conclusions: Eleven percent of patients undergoing QT autograft ACLR experienced a loss of >5° knee extension compared to the contralateral knee or required additional surgery to restore extension. QT autograft diameter and notch volume were not associated with postoperative LOE among patients who underwent primary QT autograft ACLR. The inability to achieve terminal extension (0°) at the initial preoperative presentation increased the risk of postoperative LOE by 2.23-fold and my therefore be considered as a risk factor for postoperative LOE following QT autograft ACLR rather than increased QT autograft diameter or decreased notch volume.
Figure1 [Abb. 1]
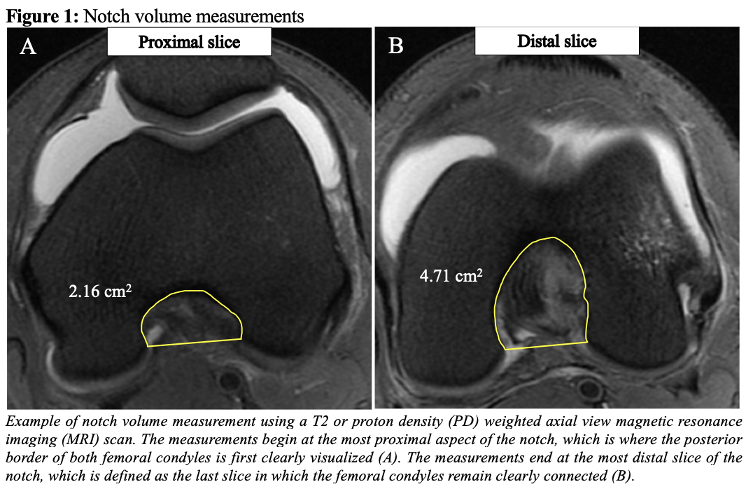
Table 1 [Tab. 1]