German Congress of Orthopaedics and Traumatology (DKOU 2025)
Lumbosacral transitional vertebrae are associated with decreased pelvic tilt but not with acetabular morphologies
Text
Objectives and questions: Lumbosacral transitional vertebrae (LSTV) are common congenital variants suspected to cause low back pain (LBP), known as Bertolotti’s Syndrome. Studies have described the effect of LSTV on acetabular orientation and pelvic tilt, but the influence on acetabular and femoral morphology remains unknown. This study aimed to determine (1) the prevalence of LSTV in patients with non-traumatic hip pain, (2) its association with patient demographic factors, (3) its association with acetabular and femoral pathology, including pelvic tilt, and (4) its association with LBP.
Material and methods: We retrospectively reviewed patients with non-traumatic hip pain between January 2010 and December 2020. Inclusion criteria were a magnetic resonance (MR) arthrogram of the hip and a computed tomography (CT) scan of the pelvis that included at least the last lumbar vertebra. Patients with traumatic hip or spine injuries, previous hip or spine surgeries, or osteoarthritis were excluded. LSTV was classified according to Castellvi’s classification based on 3D reconstruction from CT scans. Hips were classified into 10 subgroups according to femoral and acetabular morphologies. Normality was assessed using the Shapiro-Wilk test. Comparisons between groups were conducted using the Student’s t-test or the chi-squared test. Multivariate regression analysis was performed to identify predictors for LSTV. Statistical significance was set at p<0.05.
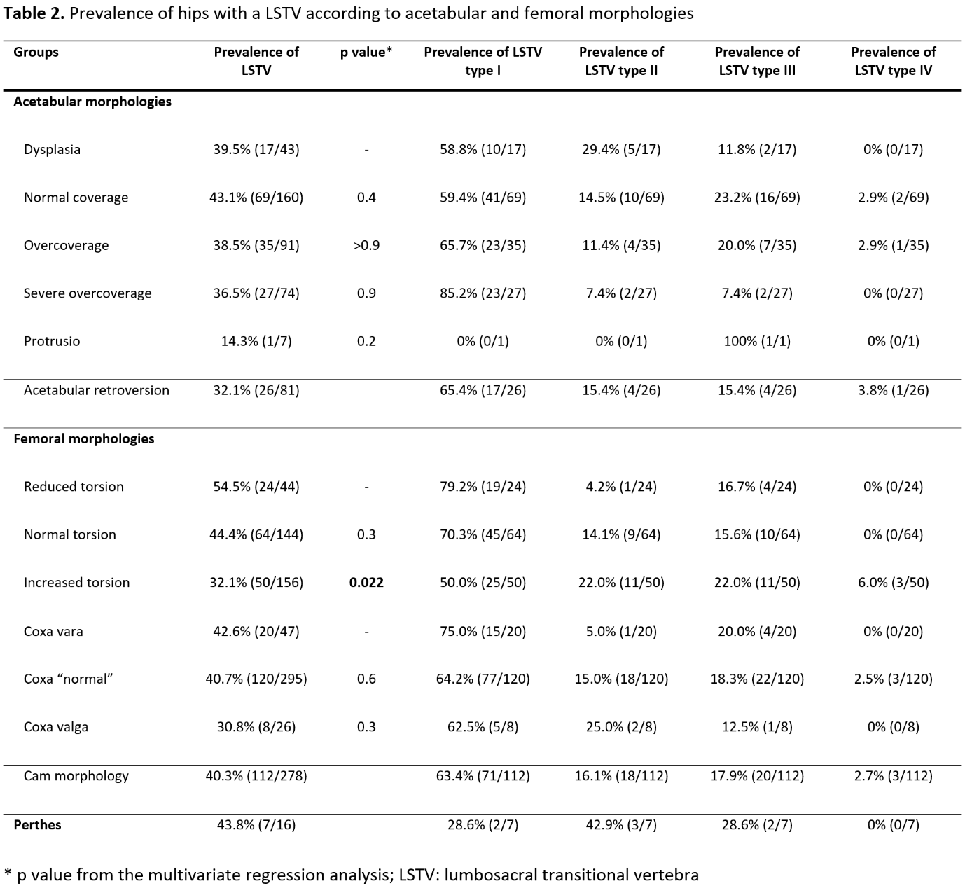
Results: 328 patients were included. (1) The overall prevalence of LSTV was 38.7%, distributed as follow: type I 65.4%, type II 15.0%, type III 18.1%, and type IV 1.6%. (2) Patients with LSTV type I were taller (1.75m ± 0.08 vs 1.70m ± 0.08, p<0.001), and more likely to be men (p<0.001) compared to patients without LSTV. (3) Patients with LSTV type III had a reduced pelvic tilt compared to those without (3.5° ± 6.2 vs 5.4° ± 5.6, p=0.018). Patients with LSTV had a decreased femoral torsion compared to those without (27.4° ± 15.9 vs 23.6° ± 13.9, p=0.017). No association was found between LSTV and acetabular morphology. (4) LSTV was not associated with LBP.
Discussion and conclusions: More than one-third of patients with non-traumatic hip pain have LSTV, with the majority being classified as type I. LSTV type I are more frequent in taller men, possibly due to the correlation between transverse process size and body size. Patients with LSTV had reduced pelvic tilt, which may influence spinal posture. However, this was not associated with an increased prevalence of LBP. No association was found between LSTV and acetabular morphology.
Figure 1 [Fig. 1]
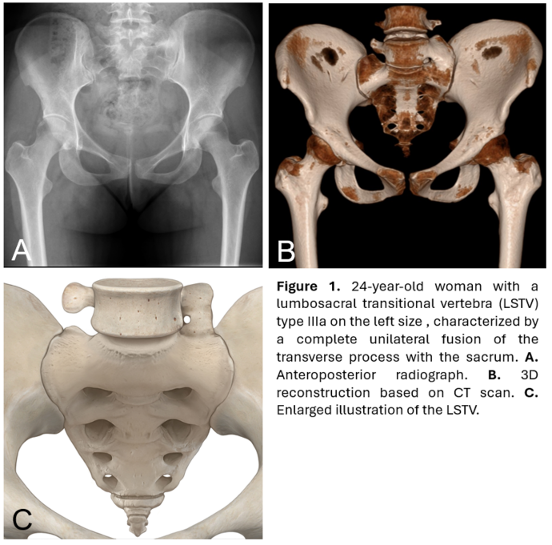
Table 1 [Tab. 1]
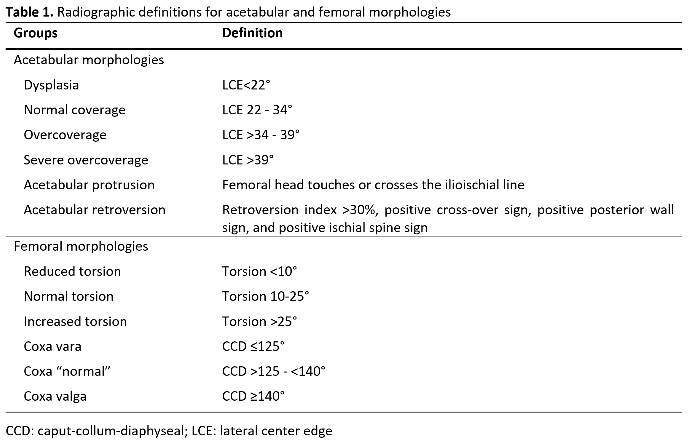
Table 2 [Tab. 2]